
GEORGIAN
BIOMEDICAL
& MEDICAL NEXUS
Former Georgian Biomedical News
ISSN (Online): 2720-8796
CASE REPORT
Prolonged Fever and Multisystem Hyperinflammation in an Adolescent Following
SARS-CoV-2 Exposure: An Atypical Multisystem Inflammatory Syndrome-Like Presentation
Eka Nakhutsrishvili1,2,4,ID, Ekaterine Uberi1,2,ID, Tamar Goginashvili3,ID, Nino Kapanadze2,ID, Elene Dolidze4,ID,
Tinatin Kutubidze1,2,4,ID
ABSTRACT
Prolonged fever with multisystem inflammation in adolescents poses a significant diagnostic challenge, especially during the viral season. Multisystem inflammatory syndrome in children (MIS-C) is a post-infectious inflammatory condition that may mimic bacterial sepsis, systemic rheumatologic disease, oncohematologic processes, or postviral dysregulation. We present a case of a 13-year-old, previously healthy boy with hectic fever, severe myalgia, and pharyngitis accompanied by elevated inflammatory markers. The clinical course was characterized by persistent fever unresponsive to broad-spectrum antibiotics, Synovitis of the knees and hips, respiratory distress with radiographic evidence of pneumonia, pericardial effusion, and mitral valve dysfunction; laboratory values include elevated cardiac troponin levels and elevated inflammatory markers (IL-6, D-dimer, and ferritin), as well as transient liver dysfunction. SARS-CoV-2 IgG was positive. Extensive infectious, hematologic, and rheumatologic evaluation was unrevealing. The patient demonstrated rapid clinical and laboratory improvement following treatment with intravenous methylprednisolone and immunoglobulin. Although the clinical picture was most compatible with MIS-C or a MIS-C-like post-SARS-CoV-2 hyperinflammatory syndrome, atypical features, including predominant respiratory involvement, gradual progression, and absence of shock, suggested a broader disease spectrum. This case highlights the diagnostic challenges of post–COVID-19 hyperinflammatory syndromes, which may present with overlapping features of infection and immune-mediated diseases.
Keywords: Adolescence; D-dimer; Hyperinflammation; IL-6; Multisystem inflammatory syndrome in children; Pediatrics; Pericardial effusion; Post-COVID immune dysregulation; Prolonged fever; Synovitis.
DOI: 10.52340/GBMN.2026.01.01.175
INTRODUCTION
Diagnosing prolonged fever in children and adolescents can be difficult, especially when early symptoms are vague and not clearly linked to a specific cause.¹ This challenge becomes even greater during seasonal viral infections, when similar symptoms can make it hard to identify the underlying cause. If the fever affects multiple body systems, such as the muscles, heart, blood, or lungs, doctors must consider a wide range of possible causes, including serious bacterial infections, autoimmune diseases, blood cancers, and immune problems that occur after infections. 1
Since COVID-19 emerged, doctors have paid closer attention to delayed-onset inflammatory illnesses in children, especially Multisystem Inflammatory Syndrome in Children (MIS-C). 2-5 MIS-C was first described during the pandemic as a severe, shock-like illness. However, it is now known to present with a range of symptoms and varying severity. 6,7 It can look like sepsis, toxic shock, or rheumatologic diseases, which makes diagnosis and treatment difficult. Differentiating postviral inflammation from a serious infection is important because treatment differs, and early diagnosis leads to better outcomes. 3,8
The exact cause of MIS-C is still not fully understood. However, it likely involves immune system problems, such as excessive cytokine release (e.g., interleukin-6 [IL-6]), impaired T-cell regulation, and abnormal immune activity. 9,10 Research suggests that molecular mimicry may play a role, in which viral proteins trigger the immune system, leading to autoimmune and vascular problems. 9,11,12 The detection of autoantibodies in patients with COVID-19 and MIS-C supports the notion that the disease has an autoimmune component. 13 Different immune profiles observed in affected children highlight the importance of immune system dysfunction in determining disease severity. 14
In addition to MIS-C, SARS-CoV-2 infection has been connected to many autoimmune and rheumatologic problems in children, such as vasculitis, juvenile idiopathic arthritis, and systemic lupus erythematosus. 11,12 This suggests that COVID-19 can trigger immune-related diseases in several ways, leading to a variety of symptoms that may change over time. In this case, we describe a difficult case involving a 13-year-old boy who had a long-lasting high fever, severe muscle pain, joint inflammation, worsening breathing problems, and heart issues. These symptoms suggested a post-SARS-CoV-2 immune-mediated process. This case demonstrates how difficult it can be to distinguish hyperinflammatory syndromes from infections and underscores the need for prompt diagnosis and collaboration among specialists.
CASES
A 13-year-old, previously healthy boy presented with a 4-day history of hectic fever, intense myalgia that even limited movement, severe sore throat with difficulty swallowing, and malaise. Upon examination, the skin appeared pale and dry, with slightly reduced turgor and elasticity, but no rash was observed. The results of vital and systemic examinations included a fever up to 39-39.7°C; rhythmic, slightly muffled cardiac tones with a regular pulse; vesicular sounds by lung auscultation and clear percussion sound; the patient's consciousness was clear, and meningeal signs were negative; by the oropharyngeal examination, hyperemic palatine arches and hypertrophic tonsils were observed; and the abdomen was soft and painless without hepatosplenomegaly.
Severe muscle pain throughout the body made it difficult to fully assess function, but muscle strength was normal (5/5). However, movement in the hip and knee joints was limited, both actively and passively.
Initial lab tests showed high inflammatory markers (CRP 100 mg/L, ESR 32 mm/hr), but the rest of the blood count was normal. Ferritin was slightly raised at 260 µg/L, and liver tests were normal. The SARS-CoV-2 antigen test was negative. Epstein–Barr virus tests showed a past infection (VCA IgG+, EBNA IgG+, IgM−). A chest X-ray and heart ultrasound were normal (FIG.1).
FIGURE 1. Chest X-ray on admission

Ultrasound of the hips and knees showed joint inflammation with mild fluid buildup. Tests for autoimmune diseases (ANA, ANCA), ASO, CK, and rheumatoid factors were all normal.
Empiric antibiotics were started, but the patient did not improve, and inflammatory markers remained elevated. Because the fever and inflammation continued, blood cultures were taken. Tests for other infections, including brucellosis, leptospirosis, borreliosis, leishmaniasis, and unusual bacteria, were all negative. The antibiotics were changed to Ceftriaxone and doxycycline, but the fever kept coming back every 6–8 hours, with severe muscle pain (especially in the left chest), and the patient's condition worsened. Blood and bone marrow tests ruled out blood cancer. Neurological exams and spinal fluid tests were normal.
Respiratory involvement progressed during hospitalization. Oxygen saturation decreased to 86–88% on room air during clinical deterioration, necessitating supplemental oxygen therapy for several days. Chest ultrasound demonstrated pleural fluid, and repeat chest radiography revealed pulmonary infiltrates, interpreted as pneumonia (FIG.2).
FIGURE 2. Repeat chest radiography

Chest CT was not performed. Although the exact etiology of the pulmonary findings could not be definitively established, the respiratory manifestations improved following immunomodulatory treatment alongside supportive care. Antibiotic treatment was still ongoing. Serial echocardiographic evaluations demonstrated pericardial effusion with a maximal thickness of approximately 10 mm and mild mitral regurgitation. Left ventricular systolic function remained preserved throughout hospitalization, with a normal ejection fraction. Coronary artery dimensions were within normal limits without evidence of coronary artery dilatation. NT-proBNP was elevated (960 pg/mL), and cardiac troponin peaked at 124 pg/mL, supporting cardiac involvement in the setting of systemic hyperinflammation. Electrocardiographic monitoring demonstrated episodes of supraventricular tachycardia (SVT), which were managed with atenolol. No significant ventricular dysfunction was identified. Laboratory findings showed further elevation of inflammatory markers (CRP 154 mg/L, procalcitonin 1.25 ng/mL) and neutrophilia with a left shift. Ceftriaxone was discontinued, and meropenem was initiated for presumed sepsis; however, the fever persisted. Blood tests showed positive SARS-CoV-2 IgG (293.4 U/mL). Following progressive multisystem involvement and increasing evidence of hyperinflammation, intravenous dexamethasone was initiated according to institutional protocols, resulting in partial clinical improvement. Given persistent fever, elevated inflammatory markers, cardiac involvement, and markedly elevated D-dimer and IL-6 levels, treatment was escalated to pulse intravenous methylprednisolone (500 mg daily for 3 consecutive days) and intravenous immunoglobulin (IVIG, 1 g/kg/day for 2 days).
Anticoagulation with enoxaparin and low-dose aspirin was initiated due to significant coagulation activation and thrombocytosis. Clinical and laboratory improvement subsequently followed, with gradual resolution of fever, respiratory symptoms, cardiac abnormalities, and inflammatory markers (SUP.TAB.1). At discharge, the patient was prescribed low-dose aspirin, atenolol, esomeprazole, and a tapering course of oral methylprednisolone. Follow-up evaluations at 1 month and 3 months demonstrated continued clinical improvement. Inflammatory markers, including CRP, had normalized, echocardiography showed complete resolution of cardiac abnormalities, and no recurrent episodes of supraventricular tachycardia were documented. Medications were gradually discontinued during follow-up, and no recurrence of fever, musculoskeletal symptoms, or hyperinflammatory manifestations was observed.
DISCUSSION
This case demonstrates the diagnostic complexity of severe hyperinflammatory syndromes in pediatric patients following COVID-19. Our observation may represent an early manifestation of a severe inflammatory response in an adolescent following remote exposure to SARS-CoV-2. The patient had no documented history of prior symptomatic COVID-19 infection. SARS-CoV-2 vaccination had not been administered because COVID-19 vaccination was not routinely available for children in his age group in Georgia during the relevant period. At admission, SARS-CoV-2 antigen testing and SARS-CoV-2 PCR were negative, whereas SARS-CoV-2 IgG antibodies were positive (293.4 U/mL), suggesting previous exposure to SARS-CoV-2. Although the exact timing of infection could not be established, the serologic findings supported prior SARS-CoV-2 exposure in the context of a hyperinflammatory multisystem illness. The initial presentation - with persistent high-grade fever, severe myalgia, and multisystem involvement - closely mimicked severe bacterial infection, underscoring the well-recognized overlap between infectious and inflammatory etiologies in pediatric practice. 1
We considered a broad differential diagnosis, including bacterial sepsis, autoimmune or autoinflammatory disease, and hematologic malignancy (TAB.1).
TABLE 1. Differential diagnosis and exclusion evidence
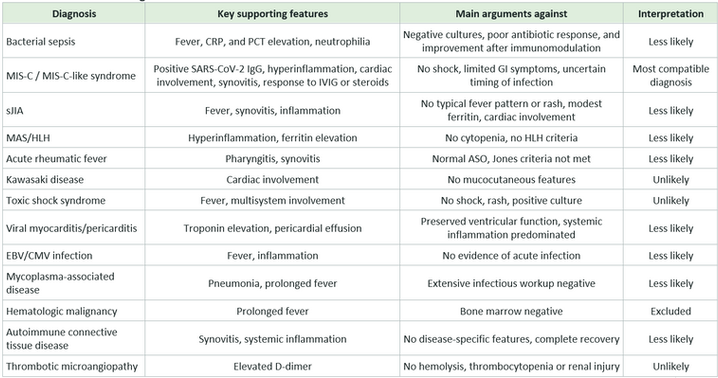
Abbreviations: ASO, Antistreptolysin O; CMV, Cytomegalovirus; CRP, C-reactive protein; EBV, Epstein-Barr Virus; HLH, Hemophagocytic Lymphohistiocytosis; IgG, Immunoglobulin G; MAS, Macrophage Activation Syndrome; MIS-C, Multisystem Inflammatory Syndrome; PCT, procalcitonin; SARS-CoV-2, Severe Acute Respiratory Syndrome Coronavirus 2; sJIA, Systemic Juvenile Idiopathic Arthritis.
Bacterial sepsis was initially the leading diagnosis given the persistent high fever and elevated inflammatory markers. However, bacterial infection became less likely because repeated microbiological investigations remained negative, no sustained response to broad-spectrum antimicrobial therapy was observed, and clinical improvement occurred only after initiation of immunomodulatory treatment. 1 Autoimmune and autoinflammatory conditions were also considered; however, the available clinical, laboratory, and imaging findings did not support these diagnoses, making them less likely. 11,12 Hematology consultation and bone marrow aspiration excluded hematologic malignancy.
From a clinical standpoint, the combination of poor response to antimicrobial therapy, negative infectious and rheumatologic workup, and rapid improvement following corticosteroids and intravenous immunoglobulin (IVIG) strongly suggests an underlying post–SARS-CoV-2 immune dysregulation.
Overall, the clinical picture is most compatible with MIS-C or a MIS-C-like post-SARS-CoV-2 hyperinflammatory syndrome (TAB.2).
TABLE 2. Mapping of patient findings to World Health Organization/CDC MIS-C criteria

This is supported by positive SARS-CoV-2 IgG, elevated inflammatory markers CRP, IL-6, ferritin, D-dimer, cardiac involvement, and Synovitis. At the same time, some features were atypical, including the delayed rise in laboratory markers and the presence of pneumonia, which are less commonly emphasized in MIS-C cohorts. 4,7,9
While the patient shares many features with MIS-C, there were also notable differences. These included the absence of shock, more prominent respiratory involvement, relatively mild gastrointestinal symptoms, and a more gradual progression of hyperinflammation rather than an abrupt onset. These outcomes support the idea that post-SARS-CoV-2 inflammatory syndromes lie along a spectrum rather than represent a single, uniform condition. 6,7
As discussed, given the possible pathophysiology of MIS-C, markedly elevated IL-6 supported the presence of a hyperinflammatory state; however, IL-6 is not specific for MIS-C and may also be elevated in severe infections and other inflammatory conditions. 9,10 Further mechanisms, such as molecular mimicry and the development of autoantibodies, further support a post-infectious autoimmune process. 11,13
In MIS-C, even mild cardiac involvement requires close monitoring. Current recommendations emphasize serial echocardiography, cardiac biomarker assessment, and rhythm monitoring during both the acute and recovery phases. In our patient, pericardial effusion, mitral regurgitation, and elevated cardiac biomarkers highlight the need for early and repeated cardiac evaluation. 15,16 Similarly, significantly elevated D-dimer levels reflect the prothrombotic state associated with MIS-C and may denote underlying endothelial injury or thrombotic microangiopathy. 17
Musculoskeletal symptoms, including severe myalgia and Synovitis, were an active part of the patient's illness and contributed to diagnostic uncertainty. Although not always described, these features can occur in postviral hyperinflammatory states and should be considered part of the clinical spectrum. 10,17
From a clinical standpoint, this case report highlights a few key concepts. First, the absence of microbiological confirmation, lack of sustained clinical response to broad-spectrum antimicrobial therapy, and subsequent improvement following immunomodulatory treatment made an immune-mediated hyperinflammatory process more likely. However, infection could not be excluded with absolute certainty. Additionally, markedly elevated IL-6 levels supported the presence of a hyperinflammatory state but were not specific to MIS-C. Its interpretation required integration with the overall clinical picture, including negative infectious investigations, cardiac involvement, coagulation abnormalities, SARS-CoV-2 serology, and the favorable response to immunomodulatory therapy. Early use of immunomodulatory therapy - particularly corticosteroids and IVIG - can significantly alter the disease course and improve outcomes. 8,14,17
To summarize, this case illustrates the heterogeneous nature of post–SARS-CoV-2 inflammatory syndromes in children. Early recognition of such atypical presentations and timely initiation of immunomodulatory treatment are essential to avoid delayed diagnosis and improve clinical outcomes.
CONCLUSIONS
This case highlights the diagnostic challenges posed by hyperinflammatory syndromes in pediatric patients following SARS-CoV-2 exposure. Our findings support the notion that post–SARS-CoV-2 immune dysregulation can present with clinical features that closely mimic severe bacterial infection, potentially delaying appropriate diagnosis and treatment.
The combination of persistent fever, multisystem involvement, elevated inflammatory markers - including IL-6 and D-dimer - and cardiac abnormalities should prompt consideration of multisystem inflammatory syndrome in children or related post-infectious hyperinflammatory states, even in the absence of shock.
From a clinical standpoint, a lack of sustained response to broad-spectrum antimicrobial therapy, negative microbiological investigations, and multisystem inflammation should raise suspicion of an immune-mediated process. Early recognition and timely initiation of immunomodulatory therapy, such as corticosteroids and intravenous immunoglobulin, are essential for improving outcomes.
In this patient, the gradual progression of respiratory involvement reinforces the view that MIS-C does not always follow a uniform clinical pattern. Recognition of atypical clinical phenotypes - such as predominant respiratory involvement, progressive hyperinflammation, and musculoskeletal manifestations - is essential for accurate diagnosis and management.
AUTHOR AFFILIATION
1 Department of Child and Adolescent Medicine, Tbilisi State Medical University (TSMU), Tbilisi, Georgia
2 Department of Pediatrics, Tbilisi State Medical University (TSMU) G. Zhvania Pediatric University Clinic, Tbilisi, Georgia
3 Department of Intensive Care Unit, Tbilisi State Medical University (TSMU) G. Zhvania Pediatric University Clinic, Tbilisi, Georgia
4 Tbilisi State Medical University American MD (USMD) Program, Tbilisi, Georgia
SUPPLEMENTARY MATERIALS
SUPPLEMENTAL TABLE 1. Clinical course

REFERENCES
-
Brogan PA, Burns JC, Cornish J, et al. The differential diagnosis of prolonged fever and systemic inflammation in children. Arch Dis Child. 2021;106(2):114-120. doi:10.1136/archdischild-2019-318909.
-
World Health Organization. Multisystem Inflammatory Syndrome in Children and Adolescents Temporally Related to COVID-19. WHO Scientific Brief. Published 2020.
-
Centers for Disease Control and Prevention. Information for Healthcare Providers About Multisystem Inflammatory Syndrome in Children (MIS-C). Published 2020.
-
Feldstein LR, Rose EB, Horwitz SM, et al. Multisystem inflammatory syndrome in U.S. children and adolescents. N Engl J Med. 2020;383(4):334-346. doi:10.1056/NEJMoa2021680.
-
Whittaker E, Bamford A, Kenny J, et al. Clinical characteristics of 58 children with a pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2. JAMA. 2020;324(3):259-269. doi:10.1001/jama.2020.10369
-
Riphagen S, Gomez X, Gonzalez-Martinez C, et al. Hyperinflammatory shock in children during the COVID-19 pandemic. Lancet. 2020;395(10237):1607-1608. doi:10.1016/S0140-6736(20)31094-1.
-
Ahmed M, Advani S, Moreira A, et al. Multisystem inflammatory syndrome in children: A systematic review. EClinicalMedicine. 2020;26:100527. doi:10.1016/j.eclinm.2020.100527
-
Henderson LA, Canna SW, Friedman KG, et al. American College of Rheumatology clinical guidance for multisystem inflammatory syndrome in children associated with SARS–CoV-2. Arthritis Rheumatol. 2020;72(11):1791-1805. doi:10.1002/art.41454.
-
Consiglio CR, Cotugno N, Sardh F, et al. The immunology of multisystem inflammatory syndrome in children with COVID-19. Cell. 2020;183(4):968-981.e7. doi:10.1016/j.cell.2020.09.016.
-
Henderson LA, Yeung RSM. MIS-C: Early lessons from immune profiling. Nat Rev Rheumatol. 2021;17:75-76. doi:10.1038/s41584-020-00566-0.
-
Zacharias H, Dubey S, Koduri G, D'Cruz D. Rheumatological complications of COVID-19. Autoimmun Rev. 2021;20(9):102883. doi:10.1016/j.autrev.2021.102883.
-
Tang KT, Hsu BC, Chen DY. Autoimmune and rheumatic manifestations associated with COVID-19: An updated systematic review. Front Immunol. 2021;12:645013. doi:10.3389/fimmu.2021.645013.
-
Burbelo PD, Castagnoli R, Shimizu C, et al. Autoantibodies against proteins associated with autoimmunity in COVID-19 and MIS-C. Front Immunol. 2022;13:841126. doi:10.3389/fimmu.2022.841126.
-
Carter MJ, Fish M, Jennings A, et al. Peripheral immunophenotypes in children with multisystem inflammatory syndrome associated with SARS-CoV-2 infection. Nat Med. 2020;26:1701-1707. doi:10.1038/s41591-020-1054-6.
-
Rowley AH. Understanding SARS-CoV-2–related multisystem inflammatory syndrome in children. Nat Rev Immunol. 2020;20:453-454. doi:10.1038/s41577-020-0367-5.
-
Belhadjer Z, Méot M, Bajolle F, et al. Acute heart failure in multisystem inflammatory syndrome in children associated with SARS-CoV-2 infection. Circulation. 2020;142:429-436. doi:10.1161/CIRCULATIONAHA.120.048360.
-
Diorio C, McNerney KO, Lambert M, et al. Evidence of thrombotic microangiopathy in children with SARS-CoV-2 across the spectrum of clinical presentations. Blood Adv. 2020;4(23):6051-6063. doi:10.1182/bloodadvances. 2020003471.