
GEORGIAN
BIOMEDICAL
& MEDICAL NEXUS
Former Georgian Biomedical News
ISSN (Online): 2720-8796
ORIGINAL RESEARCH
Pre- and Post-Pandemic Epidemiology of Rhinovirus Infections in Hospitalized Children: A Retrospective Cohort Study from Georgia
ABSTRACT
Background: Rhinoviruses are among the most common causes of acute respiratory infections in children worldwide. The COVID-19 pandemic and associated non-pharmaceutical interventions (NPIs) significantly altered the epidemiology of respiratory pathogens.
Objectives: To compare epidemiological and clinical characteristics of rhinovirus infections between the pre-pandemic (2018–2019) and post-pandemic (2023–2024) periods, assess changes in seasonal distribution, evaluate age distribution differences, and analyze clinical severity indicators.
Methods: A retrospective cohort study was conducted at M. Iashvili Central Children's Hospital, Tbilisi, Georgia. A total of 429 laboratory-confirmed rhinovirus-positive cases were analyzed: 105 from the pre-pandemic period and 324 from the post-pandemic period. Demographic characteristics, seasonal distribution, oxygen therapy, ICU admission, comorbidities, and length of hospital stay were evaluated.
Results: While rhinovirus-positive cases increased in absolute numbers post-pandemic (105 vs. 324), positivity rates did not differ significantly between periods, suggesting higher testing volume rather than a true increase in disease burden. Seasonal patterns shifted from a winter predominance (53.3%) to a more homogeneous year-round circulation, with additional peaks in spring and autumn. Age distribution differed significantly (p=0.039), with the proportion hospitalized among school-aged children increasing from 11.4% to 24.4%. Clinical severity indicators decreased, including the need for oxygen therapy (69.5% vs 40.4%; p<0.001), while ICU admission showed a non-significant reduction (25.7% vs 16.4%; p=0.057). Patients with comorbidities had longer hospital stays (median 6 vs 3 days; p<0.001).
Conclusions: The COVID-19 pandemic significantly influenced rhinovirus epidemiology among hospitalized children in Georgia, leading to increased case numbers, altered seasonal patterns, and a shift toward older age groups. Continuous surveillance and targeted preventive strategies remain essential in the post-pandemic period.
Keywords: COVID-19; Pandemic; Pediatric; Rhinovirus; Seasonal Distribution.
DOI: 10.52340/GBMN.2026.01.01.173
BACKGROUND
Rhinoviruses are among the most common respiratory pathogens worldwide and belong to the family Picornaviridae. 1,2 They represent the leading cause of acute respiratory infections across all age groups and account for a substantial proportion of outpatient visits annually. 1,3 Although traditionally regarded as mild and self-limiting infections, accumulating evidence demonstrates their association with severe respiratory complications, hospitalizations, and intensive care requirements, particularly among children, elderly individuals, and immunocompromised patients. 2,4-6
The COVID-19 pandemic significantly altered the epidemiology of respiratory pathogens, including rhinoviruses. Non-pharmaceutical interventions such as social distancing, mask use, and enhanced hand hygiene led to a marked reduction in viral circulation during 2020–2021, followed by an epidemiological rebound after relaxation of these measures. 7-10
The present study was conducted over four observational years (2018, 2019, 2023, and 2024) to analyze demographic, seasonal, and clinical characteristics of rhinovirus infections. Particular emphasis was placed on comparing the pre-pandemic and post-pandemic periods to assess potential long-term effects of COVID-19-related public health measures on rhinovirus epidemiology.
Rhinoviruses are among the most common respiratory pathogens worldwide and belong to the family Picornaviridae. 1,2 They are representing the leading cause of acute respiratory infections across all age groups and account for a substantial proportion of outpatient visits annually. 1,3 Although traditionally regarded as mild and self-limiting infections, accumulating evidence demonstrates their association with severe respiratory complications, hospitalizations, and intensive care requirements, particularly among children, elderly individuals, and immunocompromised patients. 2,4-6
The COVID-19 pandemic significantly altered the epidemiology of respiratory pathogens, including rhinoviruses. Non-pharmaceutical interventions such as social distancing, mask use, and enhanced hand hygiene led to a marked reduction in viral circulation during 2020–2021, followed by an epidemiological rebound after relaxation of these measures. 7-10
The present study was conducted over four observational years (2018, 2019, 2023, and 2024) to analyze demographic, seasonal, and clinical characteristics of rhinovirus infections. Particular emphasis was placed on comparing the pre-pandemic and post-pandemic periods to assess potential long-term effects of COVID-19-related public health measures on rhinovirus epidemiology.
In the present study, we aim to compare the epidemiological and clinical characteristics of laboratory-confirmed rhinovirus infections between the pre-pandemic period (2018–2019) and the post-pandemic period (2023–2024).
Secondary objectives of the present study were:
1. To assess changes in seasonal distribution patterns of rhinovirus infections across the study periods.
2. To evaluate differences in age and sex distribution and identify high-risk age groups for severe clinical outcomes.
3. To analyze clinical severity indicators, including oxygen supplementation, intensive care unit (ICU) admission, and the impact of underlying comorbid conditions on hospitalization duration and overall clinical outcomes.
METHODS
This retrospective cohort study was conducted at M. Iashvili Central Children's Hospital, Tbilisi, Georgia, a sentinel site for Severe Acute Respiratory Infection (SARI) surveillance under the National Center for Disease Control and Public Health of Georgia. The study included two discrete observation periods: the pre-pandemic period (January 1, 2018, to December 31, 2019) and the post-pandemic period (January 1, 2023, to December 31, 2024). The post-pandemic period was selected following the WHO declaration of the end of the COVID-19 public health emergency (May 2023); 2022 was excluded as a transitional year with residual pandemic-related disruptions to healthcare utilization and surveillance.
All hospitalized pediatric patients aged 0–18 years with laboratory-confirmed rhinovirus infection were included. Rhinovirus infection was verified by polymerase chain reaction (PCR) testing of nasopharyngeal swab specimens. Cases with co-detection of influenza and/or SARS-CoV-2 were classified as mixed infections and retained in the analysis, with rhinovirus designated as the primary pathogen. Patients with incomplete medical records or without laboratory confirmation were excluded.
Oxygen therapy was defined as supplementation initiated when SpO₂ was below 94% on room air or when clinical signs of respiratory distress were present. ICU admission was defined as transfer to the pediatric intensive care unit for respiratory failure, hemodynamic instability, or altered consciousness. Comorbidities were categorized as respiratory, cardiac, neurological, immunocompromising, or other chronic conditions.
Data were retrospectively extracted from electronic medical records and laboratory databases using de-identified patient identifiers to ensure confidentiality. Collected variables included demographic characteristics (age and sex), seasonal distribution, clinical signs and symptoms, oxygen therapy requirement, ICU admission, presence of comorbidities, length of hospital stay, and clinical outcomes. A total population sampling approach was applied, including all eligible patients during the study periods.
The final study cohort comprised 429 laboratory-confirmed rhinovirus cases: 105 cases during the pre-pandemic period and 324 cases during the post-pandemic period.
Statistical analysis was performed using IBM SPSS Statistics software (version 26.0).
Categorical variables were summarized as frequencies and percentages, while continuous variables were presented as medians and interquartile ranges (IQR).
Normality of continuous variables was assessed using the Shapiro–Wilk test. In cases of non-normal distribution, comparisons between groups were performed using the Mann–Whitney U test. Categorical variables were compared using the Pearson chi-square (χ²) test, and the strength of association was evaluated using Cramer's V coefficient. A two-tailed p-value of <0.05 was considered statistically significant.
Due to the study's retrospective design and the use of fully anonymized data, informed consent from individuals was not required. Patient confidentiality was strictly maintained throughout the study, and all data were de-identified prior to analysis.
RESULTS
During the pre-pandemic period (2018–2019), rhinovirus infection was confirmed in 105 hospitalized patients, including 33 cases in 2018 and 72 cases in 2019. Rhinovirus positivity rates were 15.2% (33/217) in 2018 and 17.7% (72/406) in 2019, with an overall prevalence of 16.9% during 2018–2019.
In the post-pandemic period (2023–2024), 324 cases were identified, including 146 cases in 2023 and 178 cases in 2024. Rhinovirus positivity rates were 23.0% (146/635) in 2023 and 15.8% (178/1,129) in 2024, with an overall prevalence of 18.4% during 2023–2024.
Comparison between the pre-pandemic and post-pandemic periods showed no statistically significant difference in prevalence (χ²=0.72, df=1, p=0.396).
During the pre-pandemic period (2018–2019), 66% (69/105) of hospitalized rhinovirus patients were male, and 34% (36/105) were female. In the post-pandemic period (2023–2024), 55% (180/324) were male, and 45% (144/324) were female, reflecting a relative increase in female hospitalizations (FIG.1).
FIGURE 1. Distribution of patients by gender
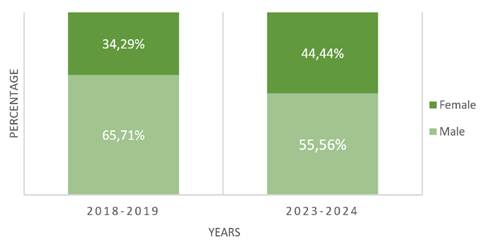
Comparison of sex distribution between the two study periods using the chi-square test showed no statistically significant difference (χ²=3.360, df=1, p=0.067). These findings indicate that the sex distribution of rhinovirus infection did not change significantly between the study periods.
The age distribution analysis of patients demonstrated significant characteristics of rhinovirus infection development in the pediatric population during the pre-COVID and post-COVID periods. During 2018-2019, the age distribution of 105 hospitalized patients with rhinovirus infection was as follows: 0–6 months - 26.6% (n=28), 6-12 months - 14.3% (n=15), 12-24 months - 24.7% (n=26), 24-60 months- 21.0% (n=22), 60-180 months - 11.4% (n=12), and >180 months (15–18 years) - 2.0% (n=2). During 2023-2024, the age structure of 324 hospitalized patients with rhinovirus infection changed and was distributed as follows: 0-6 months - 18.2% (n=59), 6-12 months - 8.6% (n=28), 12-24 months - 25.6% (n=83), 24-60 months - 20.7% (n=67), 60-180 months - 24.4% (n=79), and >180 months (15-18 years) - 2.5% (n=8) (FIG.2).
FIGURE 2. Percentage distribution of rhinoviruses in age groups

According to the χ² test, the age distribution of rhinovirus infection differed significantly between the study periods (χ²(5) = 11.724, p = 0.039). The effect size (Cramer's V=0.165) indicated a small but statistically significant association between the period factor and age groups. The test assumptions were satisfied, as only one cell (8.3%) had an expected frequency below 5.
The seasonal distribution of rhinovirus infections differed significantly between the pre-pandemic (2018–2019) and post-pandemic (2023–2024) periods (χ²(3) =61.61, p<0.001), with a moderate association between study period and seasonal patterns (Cramer's V=0.379).
During 2018–2019, the majority of cases occurred in winter (53.3%), followed by spring (21.9%), autumn (22.9%), and summer (1.9%). In contrast, during 2023–2024, winter cases decreased markedly to 17.0%, while spring cases increased to 35.8%, summer cases to 18.8%, and autumn cases to 28.4% (FIG.3).
FIGURE 3. Comparison of seasonal distribution in the pre- and post-pandemic period

Monthly analysis demonstrated a shift in peak activity from winter months in the pre-pandemic period (December 2019: 18 cases; January 2019: 14 cases) to spring and autumn peaks in the post-pandemic period (March: 53 cases; September: 46 cases). When adjusted for total SARI admissions, rhinovirus positivity rates confirmed this shift: in 2018–2019, autumn showed the highest rate (36.3%) despite fewer admissions, while in 2023-2024, rates were more evenly distributed across seasons (winter: 10.0%, spring: 21.6%, summer: 16.7%, autumn: 26.0%), excluding a testing volume artifact.
The most common reasons for hospital admission were cough, fever, and respiratory distress (FIG.4).
FIGURE 4. Distribution of patients according to clinical symptoms

During 2018–2019, 27 of 105 patients (25.7%) required ICU admission. Among these, 8 patients were treated in the neonatal ICU, and 2 were admitted to the pediatric ICU for other primary diagnoses, with rhinovirus detected as a concomitant infection. ICU patients were predominantly male (77.7%). Oxygen therapy was required more frequently in ICU patients (92.6%) than in non-ICU patients (61.5%). Pathological chest radiographic findings were observed in 74.0% of ICU patients, compared with 24.3% of non-ICU patients. Comorbid conditions were identified in 25.9% of ICU patients versus 9.6% of non-ICU patients. Co-infection with respiratory syncytial virus was detected in 7 ICU patients.
In the post-pandemic period (2023-2024), 53 of 324 patients (16.4%) required ICU admission, with 56.6% belonging to the 0-6-month age group. The gender distribution among ICU patients was 45.3% male and 54.7% female. Oxygen therapy was required in 52.8% of ICU patients compared to 33.6% of non-ICU patients. Pathological chest radiographic findings were observed in 39.6% of ICU patients, compared with 24.3% in non-ICU patients. Comorbidities were present in 35.8% of ICU patients compared to 18.5% of non-ICU patients, and RSV co-infection was detected in 9 ICU cases (FIG.5).
FIGURE 5. Distribution of patients according to oxygen consumption and ICU admission

Comparison between study periods showed that ICU admission decreased from 25.7% in 2018–2019 to 16.4% in 2023–2024, although this difference was not statistically significant (χ²=3.612, df=1, p=0.057). Oxygen therapy requirement differed significantly between periods, decreasing from 69.5% to 40.4% (χ²=26.910, df=1, p<0.001; Cramer's V=0.25).
Radiological abnormalities were significantly more frequent among ICU patients in both periods, although prevalence decreased in the post-pandemic period (74.1% vs 37.5%; p < 0.05). A sensitivity analysis was performed, including only rhinovirus cases and excluding mixed viral infections. ICU admission rates did not differ significantly between periods (χ²(1)=2.102, p=0.147; Cramer's V=0.102), indicating that co-pathogens did not materially influence the reported severity indicators.
In multivariable logistic regression, adjusting for age and sex, the study period was independently associated with the requirement for oxygen therapy. Patients in 2023-2024 had significantly lower odds of requiring oxygen therapy compared to 2018-2019 (adjusted OR=0.30, 95% CI 0.19–0.49, p<0.001). Age and sex were not significant predictors of oxygen therapy requirement.
Antibiotic use did not differ significantly between periods (52.4% vs 45.7%; χ²=1.43, p=0.232).
The Shapiro-Wilk test indicated that the length of hospitalization was not normally distributed (p<0.001). Therefore, differences between groups were assessed using the Mann-Whitney U test. The results showed that patients with comorbidities had significantly longer hospitalization (Median=6 days; Median Rank=279.5) compared to those without comorbidities (Median=3 days; Median Rank=197.4; U=9564, Z=-5.66, p<0.001).
DISCUSSION
The present study examined the epidemiology and clinical characteristics of rhinovirus infections among pediatric patients in Georgia during the pre- and post-pandemic periods. While absolute rhinovirus case numbers were higher in the post-pandemic period (105 vs. 324), positivity rates did not differ significantly (p=0.396), suggesting that increased testing volumes or altered admission patterns may partly account for this observation. Reduced exposure to respiratory pathogens during the COVID-19 pandemic may have contributed to decreased population-level immunity - the so-called immunity-debt phenomenon - though this mechanism cannot be directly tested in the present study. Alternative explanations, including changes in referral patterns, hospital admission thresholds, and healthcare-seeking behavior, should also be considered. 11-13
Our findings are consistent with international epidemiological studies that have demonstrated increased rhinovirus activity among pediatric populations following the COVID-19 pandemic. 12-14 Similar trends have been reported across multiple geographic regions. 15,16 These observations suggest that the epidemiological changes observed in Georgia reflect broader global post-pandemic patterns.
A significant shift in seasonal distribution was also observed. Before the pandemic, infections followed a classical winter-dominant pattern (53.3%), whereas post-pandemic circulation became more evenly distributed throughout the year, with additional peaks in spring and autumn. Comparable seasonal redistribution patterns have been described in European studies, particularly in association with co-circulation of respiratory syncytial virus. 17,18
Age distribution analysis revealed significant changes (p=0.039), with hospitalization rates among 5-15-year-old children rising from 11.4% to 24.4%. 12 This shift aligns with large-scale trends in China and Shenzhen-specific observations, which documented an increase in the median age of rhinovirus-positive patients from 1.83 years pre-pandemically to 3.33 years post-pandemically. 13 These findings likely reflect reduced viral exposure during school closures and the accumulation of an immunologically naïve cohort, emphasizing the need for targeted surveillance and infection prevention strategies in 5-15-year-old populations. 9,11,13,15
Indicators of disease severity appeared to decrease post-pandemic, including reduced oxygen therapy requirements (69.5% vs 40.4%, p<0.001) and a non-significant decline in ICU admissions (25.7% vs 16.4%, p=0.057).
This trend may reflect improvements in clinical management, such as earlier recognition of respiratory compromise and optimized supportive care. European surveillance studies similarly did not demonstrate increased severity following the lifting of NPIs. 17-19
Rhinovirus epidemiology differs from other respiratory viruses. Unlike RSV and influenza, which showed sharp post-NPI resurgence waves, rhinovirus maintained relatively stable circulation during the pandemic. 1,2 This pattern may be explained by intrinsic virological characteristics, including its non-enveloped structure and high serotype diversity (>160 serotypes), which limit long-term protective immunity. 1,2 These properties likely contributed to persistent circulation despite widespread public health restrictions.
From a public health perspective, continuous year-round surveillance of rhinovirus infections is essential to detect shifts in transmission dynamics. Particular attention should focus on 5-15-year-old children, who may represent an increasingly vulnerable group post-pandemic. Sustained implementation of respiratory hygiene practices, including hand hygiene and respiratory etiquette, remains important beyond the acute pandemic phase. 7-9
This study has several limitations. The retrospective design limits causal inference regarding the relationship between epidemiological changes and pandemic interventions. The single-center setting may limit generalizability; however, the study was conducted at the largest pediatric sentinel surveillance hospital in Georgia, which serves as a primary referral center for respiratory illnesses in the country, thereby enhancing the representativeness of the findings. Increased virological testing post-pandemic may have influenced detection rates. Despite these limitations, the study provides important evidence on post-pandemic shifts in pediatric rhinovirus epidemiology in Georgia. Findings contribute to international literature documenting long-term consequences of pandemic-related public health interventions. Continued monitoring of respiratory virus circulation is essential to optimize clinical preparedness and guide evidence-based public health strategies. 8,11
CONCLUSIONS
The COVID-19 pandemic significantly altered the epidemiology of rhinovirus infections among pediatric patients at Georgia's largest sentinel surveillance center, findings likely reflective of broader national trends. The post-pandemic period was marked by increased case numbers, shifts in seasonal distribution, and a transition toward older pediatric age groups, particularly 5–15-year-old school-aged children. Despite the higher case burden, indicators of disease severity declined, possibly reflecting improvements in clinical management. These findings underscore the importance of continuous surveillance of respiratory viruses and targeted preventive strategies, including hygiene measures and infection control practices, as well as vaccination programs, to address evolving transmission patterns and mitigate the long-term consequences of immunity debt in the post-pandemic era
AUTHOR AFFILIATION
1 Pediatric Department, Tbilisi State Medical University, Tbilisi, Georgia
2 Pediatric Department, M. Iashvili Central Children's Hospital, Tbilisi, Georgia
3 National Center for Disease Control and Public Health (NCDC), Tbilisi, Georgia
REFERENCES
-
Royston L, Tapparel C. Rhinoviruses and respiratory enteroviruses: not as simple as ABC. J Gen Virol. 2016;97(1):1-13. doi:10.1099/jgv.0.000334.
-
Jacobs SE, Lamson DM, St George K, Walsh TJ. Human rhinoviruses. Clin Microbiol Rev. 2013;26(1):135-162. doi:10.1128/CMR.00077-12.
-
Monto AS. Epidemiology of viral respiratory infections. Am J Med. 2002;112(suppl 6A):4S-12S. doi:10.1016/S0002-9343(01)01058-0.
-
Jartti T, Gern JE. Role of viral infections in the development and exacerbation of asthma in children. J Allergy Clin Immunol. 2017;140(4):895-906. doi:10.1016/j.jaci.2017.08.003.
-
Kim JO, Hodinka RL. Serious respiratory illness associated with rhinovirus infection in a pediatric population. Clin Diagn Virol. 1998;10(1):57–65. doi:10.1016/s0928-0197(98)00004-x.
-
Smitherman LS, et al. Rhinovirus-associated hospitalizations in young children. J Infect Dis. 2007;195(6):773–781. doi:10.1086/511982.
-
Yeoh DK, Foley DA, Minney-Smith CA, et al. The impact of COVID-19 public health measures on detections of influenza and other respiratory viruses in children in Australia. Clin Infect Dis. 2021;72(12):2199–2202. doi:10.1093/cid/ciaa1475.
-
Olsen SJ, Azziz-Baumgartner E, Budd AP, Brammer L, Sullivan S, Fasce Pineda R, Cohen C, Fry AM. Decreased influenza activity during the COVID-19 pandemic — United States, Australia, Chile, and South Africa, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(37):1305–1309. doi:10.15585/mmwr.mm6937a6.
-
Sullivan SG, Carlson S, Cheng AC, et al. Where has all the influenza gone? The impact of COVID-19 on the circulation of influenza and other respiratory viruses, Australia, March to September 2020. Euro Surveill. 2020;25(47):2001847. doi:10.2807/1560-7917.ES.2020.25.47.2001847.
-
Kuitunen I, Artama M, Mäkelä L, Backman K, Heiskanen-Kosma T, Renko M. Effect of social distancing due to the COVID-19 pandemic on respiratory tract infections in children. Pediatr Infect Dis J. 2020;39(12):e423-e427. doi:10.1097/INF.0000000000002845.
-
Cohen R, Ashman M, Taha MK, Varon E, Angoulvant F, Levy C, Rybak A, Ouldali N, Guiso N, Grimprel E. Pediatric Infectious Disease Group (GPIP) position paper on the immune debt of the COVID-19 pandemic in childhood: how can we fill the immunity gap? Infect Dis Now. 2021;51(5):418-423. doi:10.1016/j.idnow.2021.05.004.
-
Tong S, Ni Y, Liu H, Wang L. The epidemic trend of rhinovirus in children from 2013 to 2023: a large sample study in China. Ital J Pediatr. 2025;51(1):156.
-
Liu J, Wang W, Cao K, et al. Epidemiology and clinical characteristics of human rhinovirus in hospitalized children and adolescents with acute respiratory infections: a longitudinal study in Shenzhen, China (2019–2024). Virol J. 2025;22(1):280. doi:10.1186/s12985-025-02901-9.
-
Alzaydi M, Alosaimi A, Alghamdi AA, et al. Changes in seasonal respiratory viral infections among pediatric population around the COVID-19 pandemic, 2019–2023. Eur J Clin Microbiol Infect Dis. 2024;43(8):1589-1596.
-
Hatter L, Eathorne A, Hills T, Bruce P, Beasley R. Immunity debt and unseasonal childhood respiratory viruses. Br J Hosp Med (Lond). 2022;83(9):1-4.
-
Presti S, Manti S, Gambilonghi F, Parisi GF, Papale M, Leonardi S. Comparative analysis of pediatric hospitalizations during two consecutive influenza and respiratory virus seasons post-pandemic. Viruses. 2023;15(9):1825. doi:10.3390/v15091825.
-
Yang MC, Su YT, Chen PH, Tsai CC, Lin TI, Wu JR. Changing patterns of infectious diseases in children during the COVID-19 pandemic. Front Cell Infect Microbiol. 2023;13:1200617. doi:10.3389/fcimb.2023.1200617.
-
Berger A, Fruhwald T, Gerstmayr M, et al. Burden of disease and seasonal data of children hospitalized due to RSV and influenza Kurz H, Hoffmann H, Oeser R. Burden of disease and seasonal data of children hospitalized due to RSV and influenza infection before, during and after the COVID-19 pandemic. Eur J Pediatr. 2025;184(8):459. doi:10.1007/s00431-025-06289-0.
-
Kim YJ, et al. Changing trends of respiratory viruses in hospitalized children during and after the COVID-19 emergency phase in Yongin, South Korea (2020–22 vs. 2023–24). 2025.