
GEORGIAN
BIOMEDICAL
& MEDICAL NEXUS
Former Georgian Biomedical News
ISSN (Online): 2720-8796
ORIGINAL RESEARCH
Association Between Laboratory Findings and Clinical Features of Diarrheal Illness in Hospitalized Pediatric Patients Across Different Age Groups
Davit Nikolaishvili1,ID, Manana Khotchava1,2,ID, Tamar Jokhtaberidze1,2,ID, Iamze Shalamberidze1,2,ID, Mariam Rochikashvili3,ID
ABSTRACT
Background. Acute diarrheal illnesses are a common problem in the pediatric population and remain highly prevalent worldwide, especially in developing countries, where they represent one of the leading causes of mortality in children under five years of age. However, the association between the clinical severity of diarrheal illness and elevated inflammatory markers remains poorly characterized.
Objectives. To evaluate the association between laboratory findings and clinical features of diarrheal illness in hospitalized pediatric patients.
Methods. A hospital-based descriptive study was conducted among 223 hospitalized pediatric patients aged 29 days to 18 years with acute febrile diarrheal illnesses in 2025. After exclusions, the final sample comprised 190 patients. Demographic, clinical, and laboratory data were collected from medical records. Continuous variables were analyzed using the Kruskal–Wallis test, and categorical variables using Fisher’s exact test.
Results. The patients demonstrated a wide range of changes in inflammatory markers, as well as stool leukocytes and erythrocytes. Most clinical characteristics did not differ significantly across age groups; however, the number of vomiting episodes did (p=0.006), and the degree of dehydration also differed, with severe dehydration more common in infants (p=0.037). Stool erythrocyte findings were associated with the number of diarrheal episodes (p=0.003), the presence of gross blood in stool (p<0.001), and tenesmus (p<0.001). Elevated CRP levels were associated with a higher degree of fever at admission (p=0.039), and elevated ESR levels were associated with a higher number of diarrheal episodes (p=0.049). Lymphocyte levels were associated with the number of vomiting episodes (p=0.025).
Conclusions. Elevations in inflammatory markers in hospitalized children with diarrheal illnesses were variable and not uniformly associated with illness severity. However, certain laboratory findings were associated with specific clinical manifestations and may assist in clinical evaluation and management of hospitalized pediatric patients.
Keywords. C-reactive protein; Diarrheal illness; Inflammatory markers; Pediatrics; Stool erythrocytes; Stool leukocytes; White blood cell count
DOI: 10.52340/GBMN.2026.01.01.170
BACKGRUND
Diarrheal diseases are leading causes of pediatric mortality and morbidity worldwide, especially in developing countries. They are the third leading cause of death in children under five years of age, killing nearly half a million children annually.1 The clinical severity of diarrhea varies widely among pediatric patients, ranging from mild to life-threatening, as do the underlying causes of acute diarrheal conditions. While routine laboratory investigations are often not required, they play an important role in ill-appearing children and those requiring hospitalization by helping identify life-threatening etiologies and guiding clinical decision-making. These tests include complete blood count and stool studies.2 The majority of children with diarrhea are managed as outpatients after proper assessment and determination that oral rehydration therapy will be successful. Hospital admission is generally required in selected cases, such as severe dehydration or electrolyte imbalance, failure to improve with rehydration therapy, and inability to tolerate oral intake, among other indications.2 Since stool leukocytes and erythrocytes indicate intestinal mucosal inflammation, they are often assessed in hospitalized patients with diarrheal illness. Even though the diagnostic and prognostic value of these findings remains variable and context-dependent, they often influence clinical decision-making, including the initiation of empiric antimicrobial therapy.3 Due to developmental and physiological factors, inflammatory responses differ across pediatric age groups. Younger children may exhibit different laboratory abnormalities and clinical manifestations than older children, complicating their interpretation. Despite their widespread use in clinical practice, age-related differences in inflammatory marker changes and their relationship to the severity of diarrheal illness in hospitalized children remain insufficiently characterized.4 Given the frequent use of inflammatory and fecal markers in the management of children with acute diarrheal illnesses requiring hospitalization, a better understanding of their relationship with clinical severity in different age groups is needed. Such hospital-based data may help clarify their clinical relevance and improve interpretation in pediatric care.
METHODS
The hospital-based descriptive study was conducted at the Children’s Infectious Diseases Clinical Hospital in Tbilisi, Georgia, in 2025.
Study population
223 children aged from the 29th day of life up to 18 years who had been hospitalized with acute gastroenteritis, identified through review of hospital medical records.
Inclusion criteria
Hospitalized pediatric patients with acute gastroenteritis with available clinical and laboratory data, including measurements of white blood cell count, leukocyte distribution, erythrocyte sedimentation rate, C-reactive protein, stool leukocytes, and erythrocytes.
Exclusion criteria
Patients with incomplete medical records and documented coinfections were excluded to minimize confounding and allow assessment of uninfluenced laboratory findings.
Data collection
Demographic characteristics (age, sex), clinical data (degree of dehydration, duration of diarrheal disease, presence of fever), white blood cell count, leukocyte distribution, erythrocyte sedimentation rate, C-reactive protein, stool leukocytes, and erythrocytes were obtained retrospectively from the patients’ medical records.
Statistical analysis
Data were collected in Microsoft Excel and later analyzed with the Statistical Package for the Social Sciences (SPSS) version 27. Statistical analysis was performed using a statistical software package (IBM SPSS Statistics version 27.0). Continuous variables were assessed for distribution and, as they were not normally distributed, were summarized using medians and interquartile ranges (IQR), while categorical variables were presented as frequencies and percentages. Comparisons across multiple groups (age categories, stool erythrocyte groups, and laboratory parameter categories) were conducted using the Kruskal–Wallis test for continuous variables and Fisher’s exact test for categorical variables. When statistically significant differences were identified, post hoc pairwise comparisons were performed using Bonferroni correction to adjust for multiple testing. Adjusted standardized residuals were examined to identify cells contributing significantly to associations in contingency tables. All tests were two-tailed, and a p-value of less than 0.05 was considered statistically significant.
RESULTS
A total of 223 pediatric patients hospitalized with diarrheal illness were initially evaluated. Thirty-three patients were excluded due to concomitant infections, leaving 190 for the final analysis (TAB.1). The largest proportion of patients belonged to the 1–5-year age group (44.5%, n=85), followed by those aged <1 year (24.6%, n=47), 6–12 years (22.5%, n=43), and 13–18 years (7.9%, n=15).
TABLE 1. General demographics of hospitalized pediatric patients with diarrheal illness

Overall, the sex distribution was balanced, with 95 males (50.0%) and 95 females (50.0%), and remained consistent across age groups. Most patients resided in urban areas (77.9%, n=148), while 22.1% (n=42) resided in rural areas; urban residence predominated across all age categories. No statistical comparisons were performed for baseline characteristics.
Most clinical characteristics did not differ significantly across age groups, including duration of diarrhea, number of diarrheal episodes, fever at admission, and length of hospital stay (TAB.2).
TABLE 2. Clinical characteristics of hospitalized pediatric patients with diarrheal illness across different age groups

Abbreviations. IQR, interquartile range.
Note: Comparisons among age groups were performed using the Kruskal–Wallis test for continuous variables and Fisher’s exact test for categorical variables. p < 0.05 was considered statistically significant.
A statistically significant difference in the number of vomiting episodes was observed across age groups (p=0.006). Post hoc analysis with Bonferroni adjustment revealed a significant difference between children aged <1 year and those aged 6–12 years, with older children experiencing vomiting more frequently than infants (z=−3.52, p<0.001). Dehydration status also differed significantly across age groups (p=0.037). Adjusted standardized residuals showed that severe dehydration was significantly overrepresented among children aged <1 year (adjusted residual=2.3) and underrepresented among those aged 6–12 years (adjusted residual=−2.1). Conversely, moderate dehydration was significantly more frequent in the 6–12-year age group (adjusted residual=2.1) and less frequent among infants (adjusted residual=−2.3).
Most clinical characteristics did not differ significantly across stool erythrocyte groups, including fever at admission, vomiting episodes, abdominal pain, dehydration status, and length of hospital stay (all p>0.05) (TAB.3).
TABLE 3. Clinical characteristics of patients according to stool erythrocyte findings

Abbreviations. IQR, interquartile range; RBCs/HPF, Red Blood Cells per High-Power Field.
Note: Comparisons were performed using the Kruskal–Wallis test (continuous variables) and Fisher’s exact test (categorical variables). p < 0.05 was considered statistically significant.
The number of diarrheal episodes differed significantly between groups (p=0.003). Post hoc analysis with Bonferroni adjustment showed that patients with negative stool RBCs had fewer diarrheal episodes than those with numerous stool RBCs (z=−3.32, p<0.001).
Gross blood in stool was significantly more frequent in the numerous RBC group than in the few erythrocytes group (p<0.001).
Tenesmus differed significantly across stool erythrocyte groups (p<0.001). It was significantly overrepresented in the numerous stool erythrocyte group (adjusted residual=2.6) and underrepresented in those with negative stool erythrocyte (adjusted residual=−3.3), with no significant difference in the few stool erythrocyte group.
Most clinical characteristics did not differ significantly across CBC laboratory categories (normal, elevated, decreased), including WBC count, neutrophils, NLR, bands, and monocytes (all p>0.05) (TAB.4).
TABLE 4. Clinical characteristics of patients according to CBC counts
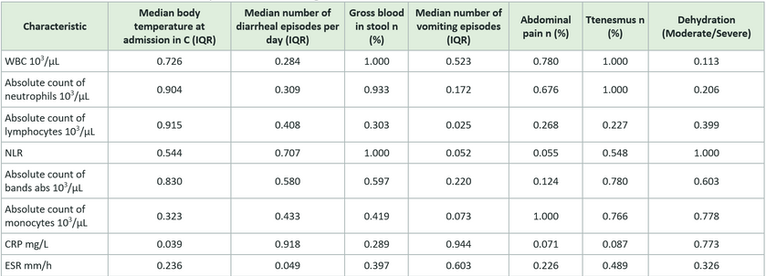
Abbreviations. CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; IQR, interquartile range; NLR, neutrophil-to-lymphocyte ratio; WBC, white blood cells.
Note: Values shown are p-values from comparisons among three laboratory groups (normal, elevated, decreased) for each clinical characteristic. Continuous variables were analyzed using the Kruskal–Wallis test and categorical variables using Fisher’s exact test. A two-tailed p < 0.05 was considered statistically significant
The number of vomiting episodes differed significantly according to lymphocyte levels (p=0.025). Post hoc analysis with Bonferroni correction showed that patients with lymphopenia had more vomiting episodes than those with normal lymphocyte counts (z=−2.65, p=0.008). Patients with markedly elevated CRP had higher fever (z=−2.42, p=0.015), and those with markedly elevated ESR had more diarrheal episodes (z=−2.60, p=0.009), after Bonferroni adjustment. (SUP.TAB.S1).
DISCUSSION
In our study, we examined clinical and laboratory characteristics of hospitalized children with acute diarrheal illnesses and analyzed how the findings differed across age groups and laboratory parameters. Most clinical characteristics were similar across age groups, which suggests that, in general, the clinical presentation of acute diarrheal illnesses does not vary significantly with age. However, we observed some important differences.
One of the differences we observed was in the number of vomiting episodes. Children aged 6-12 were more likely to experience vomiting and had more frequent vomiting episodes than infants. However, in contrast, severe dehydration was more commonly present in children under one year of age. This is a clinically meaningful finding and can be explained by the physiologic vulnerability of infants, who are more susceptible to fluid loss and dehydration due to their limited compensatory mechanisms and higher body water content.5
While many clinical features did not differ significantly between stool erythrocyte groups, the study also showed that the number of RBCs in stool remained associated with certain clinical manifestations. Patients with numerous erythrocytes in the stool had more frequent diarrheal episodes and were more likely to present with grossly visible blood in the stool and tenesmus. These findings are consistent with the understanding that the presence of stool erythrocytes may indicate intestinal mucosal inflammation or an invasive infection, which can lead to more severe gastrointestinal symptoms.6
Although most inflammatory markers were not consistently associated with the overall clinical severity of diarrheal diseases, some were. Patients with higher CRP levels had a higher fever score. Those with elevated erythrocyte sedimentation rates had more diarrheal episodes than those with normal rates. Children with lymphopenia had more vomiting episodes than those with a normal lymphocyte count. These results suggest that inflammatory markers reflect aspects of the clinical presentation of diarrheal diseases, even if they do not directly correlate with overall disease severity.4,7,8
Taken together, our findings suggest that while inflammatory markers and stool findings are not uniformly reliable indicators of disease severity, they still play an important role in the clinical evaluation of hospitalized children with diarrheal illnesses. In clinical practice, these laboratory parameters are frequent determinants of hospitalization, further monitoring, and initiation of empiric antimicrobial medications.
This study has several limitations. Firstly, it was a retrospective hospital-based study, which may limit the generalizability of the findings to outpatient populations. Second, the study included only hospitalized children, who may represent more severe cases of diarrheal illnesses. Finally, laboratory testing was performed as part of routine clinical care; therefore, not all patients may have been tested at the same stage of the illness.
Despite these limitations, this study provides useful insights into the relationships among clinical features, inflammatory markers, and stool findings in hospitalized pediatric patients with acute diarrheal illness. A better understanding of these relationships may help clinicians interpret laboratory results more appropriately and make more informed clinical decisions.
CONCLUSIONS
Inflammatory markers in hospitalized children with diarrheal illnesses exhibit variable patterns and are not consistently associated with overall clinical severity. However, certain laboratory findings, such as elevated ESR, CRP, and lymphocyte counts, and stool erythrocytes, are associated with specific clinical features, including fever, vomiting, and increased diarrheal frequency.
These findings highlight that such markers are valuable tools when interpreted alongside clinical presentation. Their appropriate use may assist clinicians in more accurate clinical evaluation, guide clinical decision-making, and support the management of hospitalized pediatric patients.
AUTHOR AFFILIATION
-
Pediatric Infectious Diseases Department, Tbilisi State Medical University, Tbilisi, Georgia
-
Children’s Infectious Diseases Hospital, Tbilisi, Georgia
-
Ken Walker International University, Tbilisi, Georgia
SUPPLEMENTARY MATERIALS
SUPPLEMENTAL TABLE S1. Clinical characteristics of patients according to complete blood count

REFERENCES
-
World Health Organization. Diarrhoeal disease. Published March 7, 2024. Accessed [date]. https://www.who.int/news-room/fact-sheets/detail/diarrhoeal-disease
-
UpToDate. Diagnostic approach to diarrhea in children in resource-abundant settings. Published 2026. Accessed January 10, 2026. https://www.uptodate.com/contents/diagnostic-approach-to-diarrhea-in-children-in-resource-abundant-settings
-
Guerrant RL, Van Gilder T, Steiner TS, et al. Practice guidelines for the management of infectious diarrhea. Clin Infect Dis. 2001;32(3):331-351. doi:10.1086/318514
-
Viviano L, Huntwork M. Inflammatory markers in pediatrics. Pediatr Rev. 2025;46(4):231-233. doi:10.1542/pir.2024-006453
-
Kliegman RM, Marcdante KJ. Nelson Essentials of Pediatrics. 8th ed. Elsevier; 2019.
-
Shane AL, Mody RK, Crump JA, et al. 2017 Infectious Diseases Society of America clinical practice guidelines for the diagnosis and management of infectious diarrhea. Clin Infect Dis. 2017;65(12):e45-e80. doi:10.1093/cid/cix669
-
Tishkowski K, Gupta V. Erythrocyte sedimentation rate. In: StatPearls. Published 2023. Accessed [date]. https://www.ncbi.nlm.nih.gov/books/NBK557485/
-
Dolin R, Reichman RC, Fauci AS. Lymphocyte populations in acute viral gastroenteritis. Infect Immun. 1976;14(2):422-428. doi:10.1128/iai.14.2.422-428.1976