
GEORGIAN
BIOMEDICAL
& MEDICAL NEXUS
Former Georgian Biomedical News
ISSN (Online): 2720-8796
ORIGINAL RESEARCH
Dermatoscopic Vascular Patterns and Invasive Tumor Depth as Predictors of Aggressive Behavior in Basal Cell Carcinoma
George Arveladze1, Rima Beriashvili1,ID, Alexander Katsitadze2,ID, Giorgi Burkadze3,ID,
Sopiko Jashiashvili4,ID, Shota Kepuladze3,ID
ABSTRACT
Background. Basal cell carcinoma (BCC) is generally characterized by indolent behavior; however, a subset of tumors demonstrates aggressive growth and recurrence. While dermatoscopy is widely used for diagnosis, its prognostic value remains insufficiently defined. This study aimed to evaluate the relationship between dermatoscopic vascular patterns and invasive tumor characteristics in BCC.
Objectives. To determine the prognostic value of dermatoscopic vascular patterns in predicting invasive growth and recurrence in basal cell carcinoma.
Methods. A retrospective cohort of 205 patients with surgically excised BCC was analyzed. Dermatoscopic features were assessed using a standardized digital imaging system, with particular emphasis on vascular morphology. Tumor size, invasive depth, histopathologic subtype, and recurrence were evaluated. Statistical analysis included non-parametric tests, correlation analysis, and Kaplan–Meier survival estimation.
Results. Polymorphous vascular patterns were strongly associated with recurrence (77% vs 8.4%, p<0.0001). Tumors with polymorphous vessels demonstrated significantly greater invasive depth (median 3.90 mm vs 1.88 mm, p<0.0001), despite smaller dermatoscopic and histologic size. These tumors were also more frequently associated with infiltrative growth, margin involvement, and perineural invasion (all p<0.01). Kaplan–Meier analysis confirmed significantly reduced disease-free survival in tumors exhibiting vascular polymorphism (p<0.0001).
Conclusions. Dermatoscopic vascular complexity, particularly polymorphous patterns, reflects invasive tumor growth and is strongly associated with recurrence in BCC. These findings suggest that dermatoscopy may serve as a clinically applicable, non-invasive tool for predicting tumor aggressiveness and guiding management.
Keywords. Basal cell carcinoma; Dermatoscopy; Prognostic markers; Recurrence; Skin cancer; Tumor depth; Tumor invasion; Vascular patterns.
DOI: 10.52340/GBMN.2026.01.01.168
BACKGROUND
Basal cell carcinoma (BCC) is the most common cutaneous malignancy and represents a significant burden in dermatologic practice.1 Although the majority of cases follow an indolent course, a subset of tumors demonstrates locally aggressive behavior, characterized by infiltrative growth, tissue destruction, and recurrence.2 Identification of such high-risk tumors remains a critical challenge, as current risk stratification is largely based on clinicopathologic parameters, including tumor size, anatomical location, and histologic subtype.3
Among these factors, infiltrative growth pattern and invasive tumor depth have consistently been associated with increased risk of recurrence.4 However, conventional assessment relies on histopathologic evaluation following excision, limiting the ability to identify aggressive tumors preoperatively. As a result, there is increasing interest in non-invasive diagnostic tools that may provide insight into tumor behavior before surgical intervention.
Dermatoscopy has become an essential method for evaluating skin tumors, enabling visualization of vascular and structural features that are not visible to the naked eye.5-7 Classic dermatoscopic criteria for BCC, such as arborizing vessels and ulceration, are well established for diagnostic purposes.8,9 However, the prognostic significance of dermatoscopic features remains less clearly defined. Emerging evidence suggests that vascular morphology may reflect underlying tumor angiogenesis and stromal interactions, processes closely linked to tumor progression.10,11
In this context, polymorphous vascular patterns, characterized by multiple vessel types within a single lesion, may serve as a marker of biologically aggressive tumor behavior. Nevertheless, the relationship between dermatoscopic vascular features and histopathologic parameters, particularly invasive tumor depth, remains underexplored.
The present study was therefore designed to investigate the association between dermatoscopic vascular patterns and invasive tumor characteristics in basal cell carcinoma. By integrating dermatoscopic findings with histopathologic and clinical data, we aim to determine whether vascular morphology can serve as a non-invasive predictor of tumor aggressiveness and recurrence.
METHODS
This study was designed as a retrospective, multicenter observational analysis of patients diagnosed with basal cell carcinoma. A total of 205 cases were retrieved from institutional pathology archives, comprising formalin-fixed, paraffin-embedded tissue specimens obtained following complete surgical excision. Inclusion criteria required the availability of complete clinicopathologic data, preoperative dermatoscopic documentation, and adequate histological material for morphometric assessment. Cases with incomplete data, inadequate tissue preservation, or absence of dermatoscopic imaging were excluded from the analysis.
Clinical data were collected from medical records and included patient age, sex, tumor location, lesion duration, and history of sun exposure. Tumor-related variables included clinical tumor size assessed by dermatoscopy, histopathologic tumor size measured on whole-slide imaging, invasive tumor depth, growth pattern, surgical margin status, and recurrence. Recurrence was defined as histopathologically confirmed reappearance of the tumor at the primary site. Follow-up time was calculated from the date of primary excision to either the date of recurrence or the last clinical evaluation.
Preoperative dermatoscopic evaluation was performed using a digital dermatoscopy system (FotoFinder Systems GmbH, Bad Birnbach, Germany), enabling standardized high-resolution imaging and reproducible documentation of lesions. Dermatoscopic images were acquired under controlled conditions and analyzed retrospectively (FIG.1). Particular emphasis was placed on vascular morphology and structural organization. Vascular patterns were classified into arborizing, polymorphous, glomerular, hairpin, and linear irregular vessels according to established dermatoscopic criteria. Polymorphous vascularity was defined as the coexistence of two or more distinct vessel types within a single lesion. Additional dermatoscopic parameters included ulceration, white shiny structures, and lesion border definition (TAB.1).
FIGURE 1. Representative dermatoscopic and histopathologic features of nodular basal cell carcinoma

Explanations: (A, D, G) Dermatoscopic images demonstrating typical features of basal cell carcinoma, including absence of pigment network, pink background, surface scaling or erosion, and arborizing or telangiectatic vessels reflecting increased vascularisation. (B, E, H) Whole-slide images (H&E, ×200) showing maximal tumor diameter. (C, F, I) Higher magnification (H&E, ×400) illustrating maximal invasive tumor depth with basaloid nests infiltrating the dermis.
TABLE 1. Association between dermatoscopic vascular patterns and tumor dimensions

Histopathological examination was performed on hematoxylin and eosin-stained sections of 3–4 μm thickness. Tumors were classified according to predominant growth pattern into nodular, superficial, and infiltrative subtypes. Special attention was given to adverse histopathologic features, including perineural invasion, lymphovascular invasion, necrosis, and surgical margin involvement (TAB.2). Tumor size was assessed using digital whole-slide imaging, and invasive tumor depth was defined as the maximum vertical extent of tumor infiltration from the epidermal surface to the deepest point of invasion.
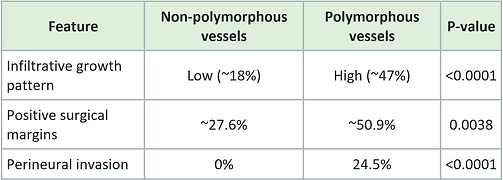
TABLE 2. Association between dermatoscopic vascular patterns and adverse histopathologic features in basal cell carcinoma
Digital slide acquisition was performed using a Motic whole-slide scanner (Motic, China). Morphometric measurements, including tumor dimensions and invasive depth, were obtained using digital image analysis tools, ensuring standardized and reproducible quantification across all cases.
The primary objective of the study was to evaluate the relationship between dermatoscopic vascular patterns and tumor depth. Secondary objectives included assessment of the association between dermatoscopic features and histopathologic aggressiveness, including infiltrative growth pattern, surgical margin involvement, and recurrence.
Statistical analysis was performed using IBM SPSS Statistics software. Continuous variables were assessed for normality using the Shapiro–Wilk test and expressed as mean ± standard deviation or median (interquartile range), as appropriate. Comparisons between groups were performed using the Mann–Whitney U test or Student's t-test for continuous variables and the chi-square or Fisher's exact test for categorical variables. Correlations among dermatoscopic tumor size, histologic tumor size, and invasive depth were evaluated using Spearman's correlation analysis.
Disease-free survival was defined as the interval between primary tumor excision and the earliest recurrence or the last follow-up. Survival curves were generated using the Kaplan–Meier method and compared using the log-rank test. A two-sided p-value of less than 0.05 was considered statistically significant.
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Tbilisi State Medical University. All patient data were anonymized before analysis.
RESULTS
A total of 205 cases of basal cell carcinoma were included in the analysis. During the follow-up period, recurrence was observed in 53 cases (25.9%), while 152 cases (74.1%) remained recurrence-free. The cohort's mean age was 61.4±10.9 years, with a median follow-up of 18 months (interquartile range, 13–29 months), allowing assessment of early and intermediate recurrence patterns.
Dermatoscopic evaluation demonstrated that vascular morphology was strongly associated with tumor behavior. Polymorphous vascular patterns were identified in a subset of lesions and were strongly associated with recurrence. All cases with polymorphous vascularity recurred, accounting for 39 of 53 recurrent tumors. In contrast, this feature was absent in the majority of non-recurrent lesions, where only 14 cases exhibited recurrence without polymorphous vascularity. This difference was highly statistically significant (p<0.0001), indicating that vascular complexity is a robust imaging correlate of aggressive tumor behavior.
Analysis of tumor dimensions revealed a non-linear relationship between surface tumor size and invasive growth. Tumors with polymorphous vascular patterns were smaller on dermatoscopy, with a median size of 4.0 mm compared to 5.0 mm in tumors lacking polymorphous vessels (p<0.05). A similar trend was observed for whole-slide imaging measurements, in which tumors with polymorphous vascularity were smaller overall (median approximately 4.5 mm versus 6.9 mm, p<0.01). In contrast, invasive tumor depth showed the opposite pattern. Tumors exhibiting polymorphous vascular patterns demonstrated significantly greater invasive depth, with a median of 3.90 mm compared with 1.88 mm in non-polymorphous lesions (p<0.0001) (FIG. 2). These findings indicate that dermatoscopic vascular complexity reflects vertical tumor growth and invasive potential rather than overall tumor size.
FIGURE 2. Dermatoscopic vascular patterns as indicators of invasive tumor behavior in basal cell carcinoma

Explanations: (A) Invasive tumor depth is significantly increased in lesions with polymorphous vascular patterns. (B) Despite a smaller dermatoscopic size, polymorphous lesions demonstrate disproportionately greater invasive depth, highlighting a discordance between surface dimensions and tumor aggressiveness.
Histopathologic analysis further supported the association between vascular patterns and aggressive tumor features. An infiltrative growth pattern was significantly more frequent in tumors with polymorphous vascularity, at approximately 47%, compared with 18% in tumors without such a pattern (p<0.0001). Similarly, surgical margin involvement was more common in polymorphous lesions (approximately 50.9% versus 27.6%; p=0.0038), suggesting a greater tendency toward subclinical extension. Perineural invasion, a well-established marker of aggressive behavior, was identified exclusively in tumors with polymorphous vascular patterns (24.5%) and was absent in tumors lacking this feature (p<0.0001).
Correlation analysis demonstrated that dermatoscopic tumor size showed only a weak relationship with invasive tumor depth, whereas vascular pattern classification provided a clearer distinction between biologically indolent and aggressive lesions. Tumors characterized by polymorphous vascularity consistently exhibited features of invasive growth, including greater depth, infiltrative architecture, and higher recurrence rates, despite their smaller superficial dimensions.
Kaplan–Meier survival analysis confirmed the prognostic significance of dermatoscopic vascular patterns. Tumors with polymorphous vessels demonstrated a markedly reduced disease-free survival compared to those without such features, with early and pronounced separation of survival curves (log-rank p<0.0001). This finding reinforces the role of vascular morphology as a clinically relevant predictor of recurrence.
Taken together, the results demonstrate that dermatoscopic vascular patterns, particularly polymorphous vascularity, are strongly associated with invasive tumor depth, adverse histopathologic features, and recurrence. Importantly, these findings indicate that tumor aggressiveness is more accurately reflected by vascular complexity and invasive growth than by overall tumor size, highlighting the potential of dermatoscopy as a non-invasive tool for risk stratification in basal cell carcinoma.
DISCUSSION
The present study demonstrates that dermatoscopic vascular morphology, particularly polymorphous vascular patterns, is strongly associated with invasive tumor growth and recurrence in basal cell carcinoma. By integrating dermatoscopic, clinicopathologic, and morphometric data, the findings provide evidence that vascular complexity represents a clinically meaningful surrogate of underlying tumor aggressiveness.
From a clinicopathologic perspective, the results are consistent with previous studies identifying an infiltrative growth pattern, margin involvement, and perineural invasion as key determinants of recurrence in basal cell carcinoma.7,12,13 These features reflect the biological capacity of the tumor to extend beyond clinically visible borders, leading to incomplete excision and local relapse. The present study extends these observations by demonstrating that such aggressive characteristics are closely linked to specific dermatoscopic vascular patterns, thereby establishing a connection between non-invasive imaging and histopathologic behavior.
A particularly important finding is the dissociation between overall tumor size and invasive growth. While tumors exhibiting polymorphous vascularity were smaller in dermatoscopic and gross histologic dimensions, they showed significantly greater invasive depth. This observation supports the notion that horizontal tumor spread does not adequately reflect biological aggressiveness, whereas vertical invasion is a more relevant predictor of clinical outcomes.14 Similar observations have been reported in recent studies emphasizing the prognostic value of tumor thickness and invasive characteristics over surface dimensions in non-melanoma skin cancers.
Dermatoscopy has long been established as a diagnostic tool for basal cell carcinoma, with characteristic features such as arborizing vessels and ulceration widely described. However, its role in prognostication has remained limited. Recent literature suggests that vascular morphology may reflect underlying tumor angiogenesis and stromal remodeling. The findings of the present study support this concept and further demonstrate that polymorphous vascular patterns are not merely descriptive but are strongly associated with invasive growth, infiltrative architecture, and recurrence. This aligns with emerging evidence indicating that vascular heterogeneity reflects dynamic tumor–microenvironment interactions and may serve as an indicator of aggressive tumor biology.11,15
In contrast, other dermatoscopic features, including ulceration and border definition, did not demonstrate significant predictive value in this cohort. This suggests that surface-level changes may be less informative than vascular architecture in assessing tumor behavior. Clinically, this distinction is relevant, as it shifts the dermatoscopic focus toward microvascular patterns, potentially enabling earlier identification of high-risk lesions before histopathologic confirmation.
The association between polymorphous vascularity and infiltrative growth pattern observed in this study further supports the hypothesis that dermatoscopic features reflect underlying structural organization. Infiltrative tumors are characterized by irregular tumor islands, stromal interaction, and subclinical extension, features that may manifest dermatoscopically as vascular complexity and heterogeneity. This relationship has been suggested in prior dermatoscopy–histopathology correlation studies, although it has not been consistently quantified.7,8
From a clinical standpoint, the results have direct implications for patient management. Current risk stratification for basal cell carcinoma relies primarily on histologic subtype and tumor size, parameters that may underestimate aggressive behavior in some cases. The present findings suggest that incorporation of dermatoscopic vascular assessment into routine evaluation could improve preoperative risk stratification. In particular, the identification of polymorphous vascular patterns may alert clinicians to the possibility of deeper invasion and a higher risk of recurrence, thereby influencing surgical planning, margin selection, and follow-up strategies.
Several limitations should be acknowledged. The retrospective design introduces potential selection bias, and the follow-up period may not capture late recurrences. Additionally, the presence of near-complete separation in some variables, particularly vascular patterns, limits the applicability of multivariate modeling. However, this phenomenon reflects the strength of the observed associations rather than a methodological limitation and underscores the potential clinical relevance of these findings.
In conclusion, the present study demonstrates that dermatoscopic vascular patterns, particularly polymorphous vascularity, are strongly associated with invasive tumor depth, adverse histopathologic features, and recurrence in basal cell carcinoma. These findings support the concept that dermatoscopy can provide not only diagnostic but also prognostic information, bridging the gap between clinical imaging and tumor biology. The integration of dermatoscopic and morphometric parameters offers a practical, clinically applicable approach to risk stratification, with the potential to improve the management of patients with basal cell carcinoma.
CONCLUSIONS
The present study demonstrates that dermatoscopic vascular patterns, particularly polymorphous vascularity, are strongly associated with invasive tumor depth and recurrence in basal cell carcinoma. These findings indicate that invasive growth characteristics more accurately reflect tumor aggressiveness than overall tumor size.
Importantly, dermatoscopic vascular complexity is a clinically accessible, non-invasive marker that correlates with underlying tumor biology. Incorporation of vascular pattern assessment into routine clinical evaluation may improve risk stratification and support more informed surgical and follow-up decisions.
AUTHOR AFFILIATION
-
Pathology Department, Tbilisi State Medical University, Tbilisi, Georgia
-
Department of Dermatology, Tbilisi State Medical University, Tbilisi, Georgia
-
Molecular Pathology Department, Tbilisi State Medical University, Tbilisi, Georgia
-
Department of Molecular and Medical Genetics, Tbilisi, Georgia
ACKNOWLEDGEMENTS
The authors acknowledge the contribution of the Department of Pathology at Tbilisi State Medical University for technical assistance and access to archival material, as well as the clinical teams involved in patient care and follow-up.
Grammarly Premium was used for language editing. No artificial intelligence tools were used for data analysis or scientific conclusions.
INFORMED CONSENT
Patient consent was waived due to the study's retrospective nature and the use of anonymized data.
ETHICAL COMPLIANCE
This study was conducted in accordance with the ethical standards of the responsible institution and with the Declaration of Helsinki. The study was approved by the Institutional Review Board of Tbilisi State Medical University (TSMU-IRB-2021/05-20).
REFERENCES
-
Verkouteren JAC, Ramdas KHR, Wakkee M, Nijsten T. Epidemiology of basal cell carcinoma: scholarly review. Br J Dermatol. 2017;177(2):359-372. doi:10.1111/bjd.15321
-
Tanese K. Diagnosis and management of basal cell carcinoma. Curr Treat Options Oncol. 2019;20(2). doi:10.1007/s11864-019-0610-0
-
Apalla Z, Nashan D, Weller RB, Castellsagué X. Skin cancer: epidemiology, disease burden, pathophysiology, diagnosis, and therapeutic approaches. Dermatol Ther (Heidelb). 2017;7(Suppl 1):5-19. doi:10.1007/s13555-016-0165-y
-
Vinicius de LV, Scapulatempo C, Perpetuo NM, et al. Prognostic and risk factors in patients with locally advanced cutaneous squamous cell carcinoma of the trunk and extremities. J Skin Cancer. 2011;2011:1-9. doi:10.1155/2011/420796
-
Yélamos O, Braun RP, Liopyris K, et al. Dermoscopy and dermatopathology correlates of cutaneous neoplasms. J Am Acad Dermatol. 2019;80(2):341-363. doi:10.1016/j.jaad.2018.07.073
-
Herzum A, Burlando M, Tavilla PP, et al. Dermatoscopically narrowed surgical margins for head and neck basal cell carcinoma: a retrospective case-control study. J Dtsch Dermatol Ges. 2022;20(6):807-816. doi:10.1111/ddg.14757
-
Sgouros D, Lallas A, Kittler H, et al. Dermatoscopic features of thin (≤2 mm Breslow thickness) vs thick (>2 mm Breslow thickness) nodular melanoma and predictors of nodular melanoma versus nodular nonmelanoma tumors: a multicentric collaborative study by the International Dermoscopy Society. J Eur Acad Dermatol Venereol. 2020;34(11):2541-2547. doi:10.1111/jdv.16815
-
Boostani M, Wortsman X, Pellacani G, et al. Dermoscopy-guided high-frequency ultrasound: principles and applications in dermatology. JID Innov. 2025;6(2):100446. doi:10.1016/j.xjidi.2025.100446
-
Nagy JA, Vasile E, Feng D, et al. VEGF-A induces angiogenesis, arteriogenesis, lymphangiogenesis, and vascular malformations. Cold Spring Harb Symp Quant Biol. 2002;67:227-237. doi:10.1101/sqb.2002.67.227
-
Ferrara N. Role of vascular endothelial growth factor in physiologic and pathologic angiogenesis: therapeutic implications. Semin Oncol. 2002;29(6 suppl 16):10-14. doi:10.1053/sonc.2002.37264
-
Boostani M, Wortsman X, Pellacani G, et al. Dermoscopy-guided high-frequency ultrasound for preoperative assessment of basal cell carcinoma lateral margins: a pilot study. Br J Dermatol. 2025;193(3):572-574. doi:10.1093/bjd/ljaf209
-
Boostani M, Bozsányi S, Suppa M, et al. Novel imaging techniques for tumor margin detection in basal cell carcinoma: a systematic scoping review of FDA- and EMA-approved imaging modalities. Int J Dermatol. 2025;64(2):287-301. doi:10.1111/ijd.17496
-
Takahashi A, Hara H, Aikawa M, Ochiai T. Dermoscopic features of small-sized pigmented basal cell carcinomas. J Dermatol. 2016;43(5):543-546. doi:10.1111/1346-8138.13173
-
Nagy JA, Vasile E, Feng D, et al. Vascular permeability factor/vascular endothelial growth factor induces lymphangiogenesis as well as angiogenesis. J Exp Med. 2002;196(11):1497-1506. doi:10.1084/jem.20021244
-
Guidi AJ, Abu-Jawdeh G, Berse B, et al. Vascular permeability factor (vascular endothelial growth factor) expression and angiogenesis in cervical neoplasia. J Natl Cancer Inst. 1995;87(16):1237-1245. doi:10.1093/jnci/87.16.1237